Shoulder replacement is the orthopedic surgery most patients in PCMC have never heard of. They know about knee replacement. They know about hip replacement. When their shoulder pain becomes severe enough to limit basic activities, they assume they will simply have to live with it. They will not. The same technology that has transformed knee and hip arthritis treats shoulder arthritis equally well.
Dr. Swaroop Solunke offers all three types of shoulder replacement at his Wakad partner hospitals in PCMC. The choice between them is not interchangeable - each is designed for a specific kind of shoulder problem. Getting the choice right is half the surgery.
What Is Shoulder Replacement?
Shoulder replacement is a procedure where the damaged surfaces of the shoulder joint (the ball at the top of the humerus and the socket of the scapula) are replaced with implant components. The implants restore smooth painless motion of the joint. Modern shoulder implants last 15 to 20 years on average.
Three Types of Shoulder Replacement
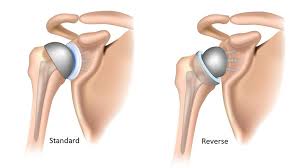
Anatomical Total Shoulder Replacement
The native ball is replaced with a metal ball on a stem and the socket is replaced with a polyethylene insert. The arrangement matches the anatomy of a normal shoulder. The rotator cuff must be intact for this implant to work.
Best for: Severe shoulder osteoarthritis or rheumatoid arthritis with intact rotator cuff. Mostly suitable for younger active patients.
Reverse Shoulder Replacement
The 'normal' anatomy is reversed. A metal ball is fixed to the socket side. A polyethylene cup is fixed to the humerus side. This design uses the deltoid muscle (the large outer shoulder muscle) to power the joint - bypassing the need for a working rotator cuff.
Best for: Severe arthritis with a torn or non-functioning rotator cuff. Cuff tear arthropathy. Massive irreparable rotator cuff tears in older patients. Complex shoulder fractures in elderly patients. Failed previous shoulder replacement.
Hemiarthroplasty (Half Replacement)
Only the ball side of the shoulder is replaced. The socket is left alone. Used when the socket is healthy but the humeral head is damaged.
Best for: Acute proximal humerus fractures in elderly patients where the head cannot be saved, or selected cases of avascular necrosis.
Why Patients Need Shoulder Replacement
Shoulder Osteoarthritis
Wear-and-tear arthritis of the shoulder joint. Causes deep aching pain, stiffness and grinding sensations. Worsens gradually over years.
Rotator Cuff Tear Arthropathy
Long-standing massive rotator cuff tears that have led to secondary arthritis. The shoulder is both arthritic and unstable. Reverse shoulder replacement is typically the right answer.
Rheumatoid Arthritis
Autoimmune inflammation that destroys the joint surface. Shoulder is commonly affected in long-standing rheumatoid arthritis.
Avascular Necrosis of the Humeral Head
Loss of blood supply causes the bone of the humeral head to die and collapse. Causes include long-term steroid use, alcohol use, sickle cell disease and previous shoulder injury.
Severe Proximal Humerus Fractures
Complex four-part fractures in elderly patients with poor bone quality often heal poorly with fixation. Reverse shoulder replacement gives a much better functional outcome in this group.
Failed Previous Shoulder Surgery
Failed rotator cuff repair, failed instability surgery, failed previous shoulder replacement - revision surgery often involves shoulder replacement.

How Shoulder Replacement Is Performed
Under regional or general anesthesia. The patient is positioned in a semi-sitting beach-chair position or on the side. A 10 to 15 centimetre incision is made over the front of the shoulder.
The surgeon enters through the deltopectoral interval, identifies the rotator cuff and exposes the joint. The damaged humeral head is removed. The socket is reshaped (or a metal sphere is placed for reverse replacement). The humeral component is fixed to the upper arm bone using bone cement or a press-fit stem. Trial components confirm fit and stability before final implants are placed.
The wound is closed in layers. The arm is placed in a sling. Total surgery time: 90 to 150 minutes.
Pricing for Shoulder Replacement in Pune
- Anatomical total shoulder replacement: Rs. 2 to 3 lakh excluding implant
- Reverse shoulder replacement: Rs. 2.2 to 3.5 lakh excluding implant
- Hemiarthroplasty: Rs. 1.5 to 2.2 lakh excluding implant
- Implant cost (additional): Rs. 1.5 to 4 lakh depending on brand and type
- Hospital stay: 3 to 5 days
Typical total inclusive bill range: Rs. 4 to 7 lakh. Insurance plans typically cover shoulder replacement on cashless basis.
Recovery After Shoulder Replacement
Week 1 to 4
Arm in a sling. Passive range of motion only - the physiotherapist moves the arm, the patient does not lift it actively. Pain control with oral medication. Discharge typically on day 3 or 4.
Week 4 to 8
Sling discontinued for most activities. Active assisted range of motion. Light pendulum and table-top exercises.
Week 8 to 12
Active range of motion against gravity. Initial light resistance exercises.
Month 3 to 6
Progressive strengthening. Return to overhead activities. Most patients regain enough function to drive, shop, do household tasks and reach overhead by month 4 to 6.
What Patients Can Do After Shoulder Replacement
- Drive, cook, shop, dress and bathe independently
- Reach overhead shelves and combs
- Light gym exercises and swimming
- Walking sports - golf, light doubles tennis, recreational cricket fielding
- Yoga with modifications
- Carry shopping bags up to 5 to 8 kg in the operated arm
Activities to Avoid After Shoulder Replacement
- Heavy weight lifting above 10 kg
- Contact sports with risk of falling on the shoulder
- Repeated heavy overhead work (manual labour, painting ceilings)
- Throwing sports at competitive intensity
